Shoulder repair for a rotator cuff is very similar to the repair of a labral tear. The athlete will go through a long, arduous recovery that will test their patience and fortitude. The shoulder is a very complex joint that utilizes many muscles which include the rotator cuff. The rotator cuff consists of tendons that allow the shoulder to externally and internally rotate and provides the dynamic glenohumeral stability needed to move the shoulder in all the directions that it is capable of moving. Because of the overall complexity of the joint and the rotator cuff, it is important that the athlete follows a strict protocol that will be created by the surgeon and managed by the physical therapists that will contain the phases of recovery for the athlete.18
The first phase happens within the first two weeks of surgery. This phase is not very strenuous, it involves passive range of motion (PROM) exercises that the athlete can tolerate. One of these exercises are usually pendulum swings, where the athlete slightly bends over and allows their arm to hang. The athlete then uses their body to gently rock the arm back and forth. The athlete can also begin to do non-resistive active range of motion (AROM) exercises with the elbow and wrist. When the athlete is not doing these exercises, they should always be wearing their sling at all times and also icing their shoulder as much as possible.19


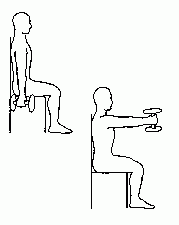
The next phase is week 2-6 after surgery and this is usually when the athlete will begin to make regular visits to the physical therapist office. The athlete continues to do the same exercises they were doing in the first phase and also add shoulder pulleys. Shoulder pulleys involve a pulley system with a rope and handles at each end. The athlete then sits in a chair and uses their non-surgery arm to lift their surgery arm as high as they can tolerate or the range that the therapists allows. The athlete also does a few isometric exercises in which they will bend their arm and gently push their fist or elbow into a wall. The athlete will begin to perform active assistive range of motion exercises (AAROM) in which the athlete will use a cane to move their arm in different motions that the therapists has approved. The athlete will begin to do gentle scapular squeezes to help build a little strength in the shoulder blades. During all these exercises the therapists will help the athlete to be aware of their posture by reminding the athlete to keep their shoulder down and back while doing these exercises. The therapists will also perform manual therapy if needed. During manual therapy the therapists uses their hands to increase the range of motion on the shoulder. The athlete should only wear the sling at night and in uncontrolled situations while icing as much as possible.19


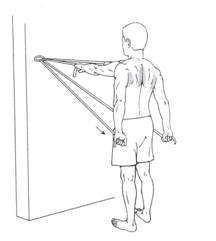
Phase three is week 6-12. The athlete no longer has any limits on the previous exercises. They can now use the cane to move their shoulder in any direction, they can use the pulleys to bring their arm as high as they can, and they can perform all the isometric exercises. The therapists will also begin the use of therabands and AROM exercises like shoulder flexion to help stabilize and strengthen the shoulder. The therapists will constantly preach postural awareness to the athlete while they do these exercises. The athlete will no longer need to wear the sling but will still need to be careful that they do not put the arm in any dangerous positions.19
Phase four is from week 12-18. The athlete will no longer need to do range of motion exercises and isometric exercises, but they will do more theraband exercises and plyometric exercises such as the ball toss. The athlete will do more dumbbell exercises and the therapists will utilize other machines in the office that will help build shoulder strength and stability. In this phase the athlete will begin to work themselves slowly back into their team weight room program and sports activities.19
References
18Meijden, O. A., Westgard, P., Chandler, Z., Gaskill, T. R., Kokmeyer, D., & Millett, P. J. (n.d.). Rehabilitation After Arthroscopic Rotator Cuff Repair: Current Concepts Review and Evidence-Based Guidelines. Retrieved March 20, 2016, from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3325631/
19Rotator Cuff Repair Rehabilitation Protocol. (n.d.). Retrieved March 20, 2016, from http://www.orthoassociates.com/SP11B4/